
Many people use the terms celiac disease, gluten sensitivity, and gluten intolerance as if they mean the same thing.
They do not.
Both conditions can cause bloating, abdominal pain, diarrhea, fatigue, brain fog, and discomfort after eating foods that contain gluten. But the reason behind the symptoms is different. That difference matters because celiac disease can damage the small intestine, interfere with nutrient absorption, and require lifelong strict gluten avoidance.
Gluten sensitivity can also affect quality of life, but it does not cause the same autoimmune injury to the small intestine. The National Institute of Diabetes and Digestive and Kidney Diseases explains that gluten sensitivity may cause symptoms similar to celiac disease, but unlike celiac disease, it does not damage the small intestine.
This is why patients should avoid self-diagnosing too quickly. If you remove gluten before testing, celiac disease can become harder to confirm. A gastroenterologist can help decide whether symptoms are caused by celiac disease, non-celiac gluten sensitivity, wheat allergy, irritable bowel syndrome, inflammatory bowel disease, lactose intolerance, or another digestive condition.
What Is Celiac Disease?
Celiac disease is a chronic digestive and immune disorder triggered by eating gluten. Gluten is a protein found in wheat, barley, and rye.
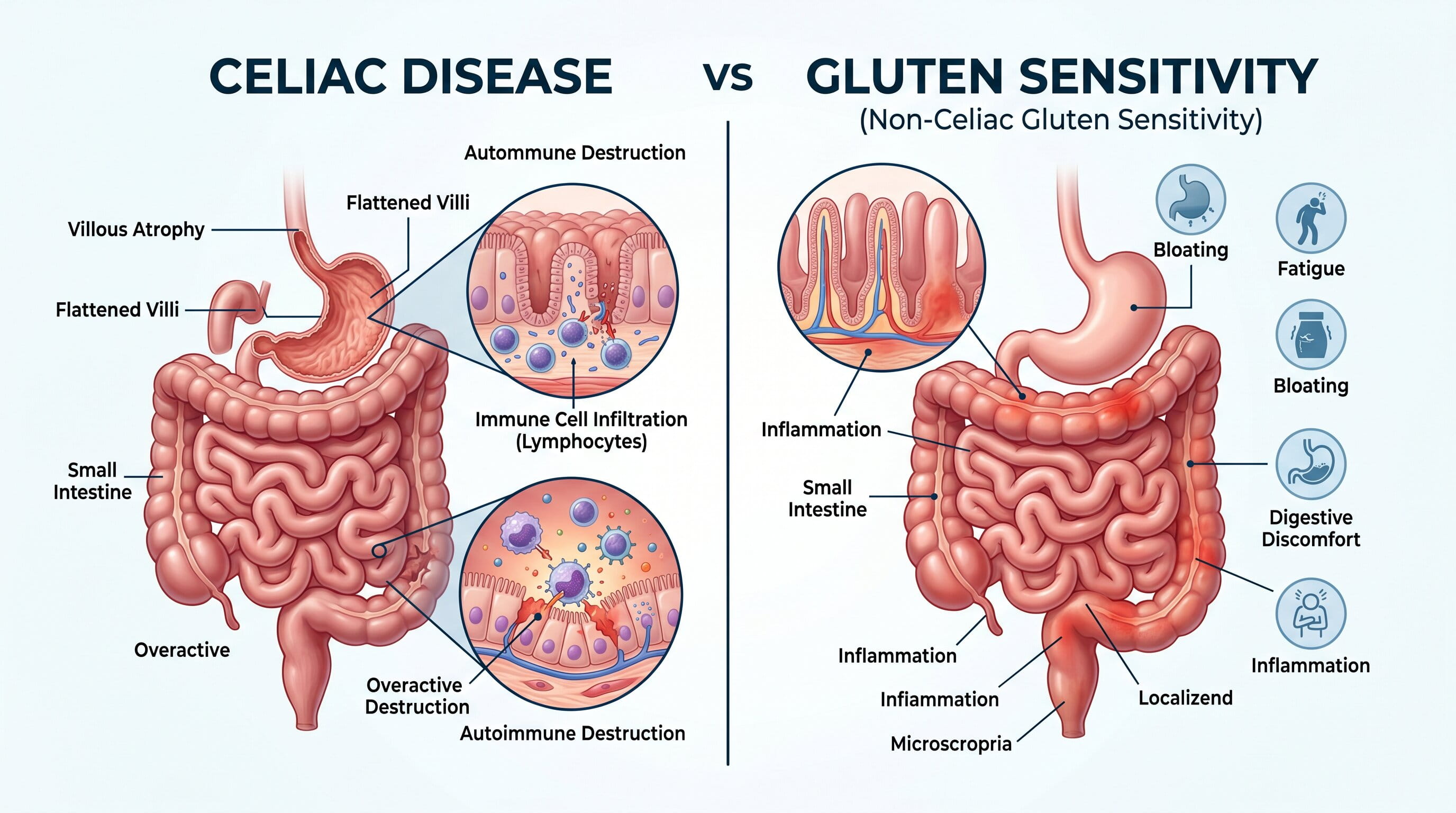
In people with celiac disease, gluten causes the immune system to attack the lining of the small intestine. Over time, this can damage the villi, which are tiny finger-like structures that help absorb nutrients from food.
When the small intestine is damaged, the body may not absorb iron, calcium, vitamin D, folate, B vitamins, and other nutrients properly. This can lead to digestive symptoms and problems outside the gut.
NIDDK describes celiac disease as a chronic digestive and immune disorder that damages the small intestine and can prevent the body from getting all the nutrients it needs.

What Is Gluten Sensitivity?
Gluten sensitivity, more accurately called non-celiac gluten sensitivity, is a condition in which a person develops symptoms after eating gluten-containing foods but does not have celiac disease or wheat allergy.
The symptoms may feel very real. A person may experience bloating, gas, abdominal pain, diarrhea, constipation, fatigue, headaches, or brain fog after eating bread, pasta, baked goods, or other gluten-containing foods.
However, non-celiac gluten sensitivity does not show the same autoimmune blood markers or small-intestinal biopsy damage seen in celiac disease. The American College of Gastroenterology notes that non-celiac gluten sensitivity can cause digestive symptoms after gluten exposure, but blood tests and tissue tests do not show celiac disease.
The Main Difference Between Celiac Disease and Gluten Sensitivity
The biggest difference is intestinal damage.
Celiac disease can damage the small intestine. Gluten sensitivity does not cause the same type of autoimmune intestinal injury.
That one difference changes everything: testing, treatment strictness, follow-up care, nutritional monitoring, and long-term risk.
| Feature | Celiac Disease | Gluten Sensitivity |
|---|---|---|
| Immune reaction | Autoimmune response | Not the same autoimmune process |
| Small intestine damage | Yes, possible | No typical celiac-type damage |
| Blood tests | Often positive when eating gluten | Usually negative for celiac markers |
| Biopsy findings | May show villous damage | No celiac-type villous damage |
| Nutrient deficiency risk | Higher | Usually lower |
| Treatment | Lifelong strict gluten-free diet | Gluten reduction or avoidance based on symptoms |
| Medical follow-up | Important | Based on symptoms and clinical judgment |
Why This Difference Matters
It may seem easier to simply stop eating gluten and see if symptoms improve. But this approach can create problems.
If you have undiagnosed celiac disease and start a gluten-free diet before testing, your antibody levels may fall and your intestinal lining may begin to heal. This can make blood tests and biopsies less accurate.
That means you may never know whether you have a lifelong autoimmune condition or a sensitivity pattern.
This matters because celiac disease needs more than symptom control. It may require:
- Strict lifelong gluten avoidance
- Nutritional deficiency testing
- Bone health evaluation in some patients
- Family screening when appropriate
- Follow-up bloodwork
- Monitoring for persistent symptoms
- Dietitian guidance
Gluten sensitivity usually does not require the same level of medical surveillance.
Symptoms That Can Overlap
Celiac disease and gluten sensitivity can look very similar at first.
Both may cause:
- Bloating
- Gas
- Abdominal pain
- Diarrhea
- Constipation
- Nausea
- Fatigue
- Headaches
- Brain fog
- Joint discomfort
- General discomfort after eating gluten-containing foods
NIDDK lists bloating, chronic diarrhea, constipation, gas, nausea, vomiting, and abdominal pain among possible celiac disease symptoms.
Because these symptoms overlap, symptoms alone are not enough to confirm which condition you have.
Symptoms That May Point More Toward Celiac Disease
Some symptoms and findings raise stronger concern for celiac disease, especially when they are persistent or unexplained.
These include:
- Iron deficiency anemia
- Unexplained weight loss
- Chronic diarrhea
- Greasy or foul-smelling stools
- Fatigue with low nutrient levels
- Mouth ulcers
- Low vitamin D
- Bone thinning or early osteoporosis
- Infertility or recurrent pregnancy loss
- Elevated liver enzymes without a clear cause
- Dermatitis herpetiformis, a blistering itchy rash
- Family history of celiac disease
- Other autoimmune conditions
Mayo Clinic notes that dermatitis herpetiformis is a blistering skin condition associated with gluten intolerance and is often linked with small-intestinal changes seen in celiac disease.
If any of these are present, it is especially important not to dismiss symptoms as simple gluten intolerance.
Symptoms That May Point More Toward Gluten Sensitivity
Gluten sensitivity may be more likely when symptoms occur after gluten exposure but celiac disease testing and wheat allergy testing are negative.
Patients may report:
- Bloating after wheat-based meals
- Abdominal discomfort without nutrient deficiencies
- Fatigue or brain fog after eating gluten
- Symptoms that improve when gluten is reduced
- No evidence of small-intestinal damage
- No celiac antibodies on appropriate testing
However, gluten sensitivity can still be difficult to define. Some people who believe they react to gluten may actually be reacting to other wheat components, fermentable carbohydrates, food additives, or an underlying digestive disorder.
This is one reason a structured evaluation is better than guessing.
Can You Tell the Difference at Home?
Not reliably.
You may notice that bread, pasta, pizza, crackers, or baked goods trigger symptoms. But that does not prove celiac disease or gluten sensitivity.
Several conditions can mimic gluten-related symptoms, including:
- Irritable bowel syndrome
- Lactose intolerance
- Small intestinal bacterial overgrowth
- Inflammatory bowel disease
- Wheat allergy
- Fructan intolerance
- Functional dyspepsia
- Pancreatic or bile-related digestive problems
- Medication-related GI symptoms
A person may blame gluten when the real trigger is wheat fermentable carbohydrates, dairy, high-fat meals, stress, or another digestive condition.
Why Testing Should Come Before Going Gluten-Free
This is one of the most important points in the entire article.
If celiac disease is possible, testing should usually be done while the person is still eating gluten. Removing gluten too early can reduce the immune response that tests are designed to detect.
Celiac testing may include:
- Tissue transglutaminase IgA antibody test
- Total IgA level
- Additional antibody testing when needed
- Upper endoscopy with small-intestinal biopsy in selected cases
- Genetic testing in certain situations
Mayo Clinic states that blood tests can help diagnose celiac disease, including serology testing for antibodies and genetic testing for related genes.
A gastroenterologist can decide which tests are appropriate based on symptoms, diet history, family history, and current gluten intake.
How Celiac Disease Is Diagnosed
Celiac disease diagnosis usually begins with a medical history and blood tests. If blood tests suggest celiac disease, an upper endoscopy with small-intestinal biopsy may be recommended.
During an upper endoscopy, a thin flexible tube with a camera is used to examine the upper digestive tract. Small tissue samples can be taken from the small intestine to check for villous damage.
Diagnosis may involve:
- Reviewing symptoms and family history
- Confirming whether the patient is currently eating gluten
- Ordering celiac antibody blood tests
- Considering upper endoscopy and biopsy
- Checking for nutritional deficiencies
- Creating a long-term gluten-free care plan if confirmed
The American College of Gastroenterology guideline focuses on diagnosis, management, and follow-up of celiac disease in adults and children, reflecting that this condition requires structured medical evaluation rather than guesswork.
How Gluten Sensitivity Is Diagnosed
There is no single confirmed blood test or biopsy that proves non-celiac gluten sensitivity.
Instead, diagnosis is usually made after:
- Celiac disease is ruled out
- Wheat allergy is ruled out
- Other digestive conditions are considered
- Symptoms improve when gluten is removed
- Symptoms return when gluten is reintroduced
This is called a diagnosis of exclusion.
A review published in JAMA describes non-celiac gluten sensitivity as symptoms related to gluten-containing grains in people who do not have celiac disease or wheat allergy, with improvement when those foods are removed.
Because there is no single definitive test, working with a GI specialist can prevent mislabeling the condition.
Is Gluten Sensitivity Less Serious Than Celiac Disease?
In terms of intestinal damage and long-term autoimmune risk, gluten sensitivity is generally less concerning than celiac disease.
But that does not mean symptoms should be ignored.
Ongoing bloating, diarrhea, constipation, abdominal pain, fatigue, or unexplained digestive distress still deserves evaluation. Even if celiac disease is ruled out, symptoms may be caused by another treatable digestive disorder.
The goal is not just to label the problem. The goal is to understand why symptoms are happening.
Can Gluten Sensitivity Turn Into Celiac Disease?
Gluten sensitivity is not generally considered an early stage of celiac disease.
However, symptoms can change over time. A person who previously tested negative may need repeat evaluation if they develop new red flags such as anemia, weight loss, chronic diarrhea, malnutrition, or a strong family history.
If symptoms worsen or new signs appear, it is worth seeing a gastroenterologist rather than assuming the diagnosis is unchanged.
What Foods Contain Gluten?
Gluten is commonly found in:
- Wheat
- Barley
- Rye
- Bread
- Pasta
- Cakes
- Cookies
- Crackers
- Cereals
- Beer
- Flour tortillas
- Breading
- Some sauces and gravies
- Some processed foods
Hidden gluten can appear in foods that do not seem obvious. This matters especially for confirmed celiac disease, where even small exposures may trigger immune activity.
Is a Gluten-Free Diet the Same for Both Conditions?
Not exactly.
For confirmed celiac disease, the gluten-free diet must be strict and lifelong. Even small amounts of gluten can matter.
For gluten sensitivity, the level of avoidance may vary. Some people feel better with complete avoidance. Others tolerate small amounts. The approach depends on symptom response and medical guidance.
The American College of Gastroenterology states that the only effective treatment for celiac disease is a strict gluten-free diet.
Common Mistake: Starting a Gluten-Free Diet Too Early
Many patients feel frustrated by symptoms and remove gluten before seeing a doctor. This is understandable, but it can delay diagnosis.
The problem is simple: celiac tests work best when the immune system is actively reacting to gluten. If gluten has already been removed, test results may look normal even if celiac disease was previously active.
Before making major diet changes, it is better to talk to a healthcare professional, especially if symptoms are chronic or severe.
Common Mistake: Assuming Gluten Is Always the Problem
Gluten gets blamed for many digestive symptoms, but it is not always the cause.
For example, wheat also contains fructans, a type of fermentable carbohydrate that can trigger bloating and gas in people with IBS. Dairy, artificial sweeteners, high-fat foods, carbonated drinks, stress, and meal timing can also contribute to symptoms.
A careful symptom history can help separate gluten-related symptoms from other digestive triggers.
When to See a Gastroenterologist
You should consider seeing a gastroenterologist if you have symptoms after eating gluten and also have:
- Chronic diarrhea
- Persistent bloating
- Abdominal pain that keeps returning
- Unexplained weight loss
- Iron deficiency anemia
- Fatigue with low nutrient levels
- Frequent nausea
- Greasy or foul-smelling stools
- Family history of celiac disease
- Other autoimmune conditions
- Symptoms that do not improve with basic diet changes
For patients in the Houston, Cypress, Katy, or Jersey Village area, GastroDoxs can evaluate persistent digestive symptoms and help determine whether celiac disease testing, endoscopy, lab work, or another GI evaluation is appropriate.
Why Celiac Disease Should Not Be Missed
Untreated celiac disease can lead to ongoing inflammation and nutrient absorption problems.
Possible complications may include:
- Iron deficiency anemia
- Vitamin deficiencies
- Bone loss
- Weight loss
- Fertility-related concerns
- Neurologic symptoms in some patients
- Persistent digestive symptoms
- Poor quality of life
Cleveland Clinic notes that ongoing inflammation from celiac disease can damage the intestine and make it hard to get enough nutrients from food.
Early diagnosis can help patients begin the right diet and reduce the risk of long-term complications.
Practical Next Steps If You Suspect Gluten Is a Problem
If you think gluten is causing symptoms, do not rush into a long-term gluten-free diet without a plan.
A better approach is:
- Write down symptoms and food triggers
- Note whether symptoms happen after wheat, dairy, fatty meals, or other foods
- Do not remove gluten before testing unless advised
- Ask your doctor about celiac blood testing
- See a gastroenterologist if symptoms are persistent
- Consider endoscopy if recommended
- Work with a dietitian if celiac disease is confirmed
This approach protects diagnostic accuracy and helps avoid unnecessary food restriction.
Final Answer: Celiac Disease vs Gluten Sensitivity
Celiac disease and gluten sensitivity can feel similar, but they are not the same condition.
Celiac disease is an autoimmune disorder that can damage the small intestine and affect nutrient absorption. Gluten sensitivity causes symptoms after eating gluten-containing foods but does not cause the same autoimmune intestinal damage.
The safest step is to get evaluated before removing gluten from your diet. Testing can help confirm whether symptoms are due to celiac disease, gluten sensitivity, wheat allergy, IBS, or another digestive condition.
For ongoing bloating, diarrhea, constipation, abdominal pain, fatigue, anemia, or unexplained weight changes, a gastroenterologist can help identify the cause and guide the right treatment plan.


