
Celiac disease can be difficult to diagnose because its symptoms often look like other digestive problems.
A person may have bloating, diarrhea, constipation, abdominal pain, nausea, fatigue, low iron, weight loss, or brain fog. These symptoms can overlap with irritable bowel syndrome, lactose intolerance, gluten sensitivity, inflammatory bowel disease, food intolerance, and other GI conditions.
That is why celiac disease should not be diagnosed by symptoms alone.
A proper diagnosis usually includes a medical history, blood tests, and sometimes an upper endoscopy with small-intestinal biopsy. The National Institute of Diabetes and Digestive and Kidney Diseases states that doctors most often use blood tests and small-intestinal biopsies to diagnose or rule out celiac disease.
The most important rule is this: do not stop eating gluten before testing unless your doctor tells you to.
If gluten is removed too early, test results may become less accurate.
Why Celiac Disease Needs Proper Diagnosis
Many patients try a gluten-free diet before getting tested. Some feel better and assume they have celiac disease. Others feel no change and assume gluten is not the problem.
Both conclusions can be wrong.
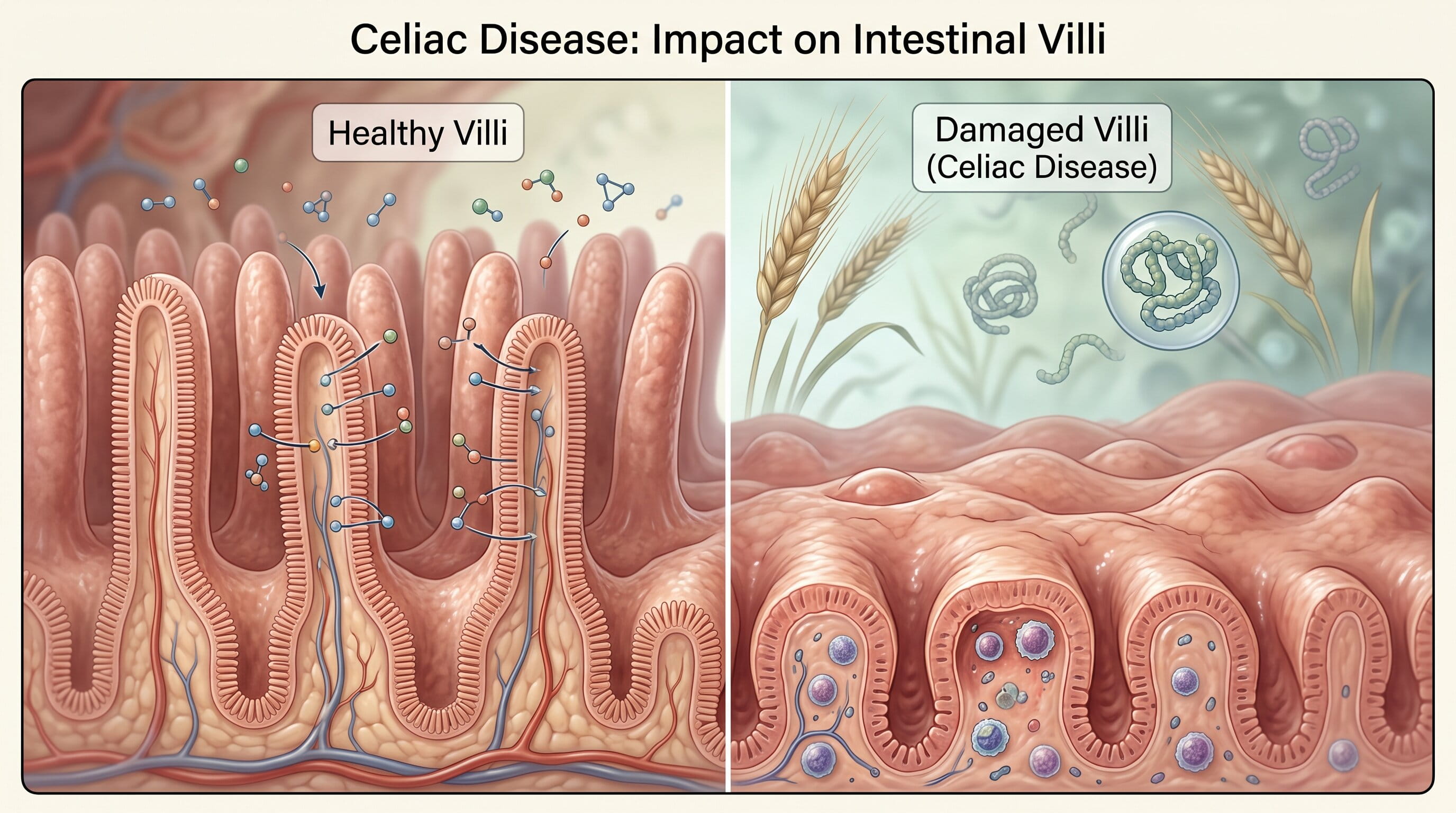
Celiac disease is an autoimmune condition. When someone with celiac disease eats gluten, the immune system reacts and damages the small intestine. This can reduce nutrient absorption and lead to iron deficiency, vitamin deficiencies, fatigue, bone loss, and other long-term problems.
A confirmed diagnosis matters because celiac disease requires lifelong strict gluten avoidance and medical follow-up.
Without proper testing, a patient may not know whether they have:
- Celiac disease
- Non-celiac gluten sensitivity
- Wheat allergy
- Irritable bowel syndrome
- Lactose intolerance
- Inflammatory bowel disease
- Small intestinal bacterial overgrowth
- Another digestive condition
This distinction is important because each condition is managed differently.
Step 1: Medical History and Symptom Review
Diagnosis begins with a detailed symptom history.
A gastroenterologist may ask about:
- Bloating
- Diarrhea
- Constipation
- Gas
- Abdominal pain
- Nausea
- Vomiting
- Fatigue
- Weight loss
- Iron deficiency anemia
- Low vitamin D
- Mouth ulcers
- Skin rashes
- Headaches
- Brain fog
- Family history of celiac disease
- Other autoimmune conditions
- Current gluten intake
The doctor may also ask whether symptoms happen after eating wheat, bread, pasta, baked goods, cereal, or processed foods.
However, symptoms alone cannot confirm celiac disease.
Some people with celiac disease have strong digestive symptoms. Others mainly have non-digestive signs like anemia, fatigue, infertility concerns, osteoporosis, or abnormal liver enzymes.
Step 2: Confirm Whether You Are Eating Gluten
Before ordering tests, the doctor needs to know whether you are still eating gluten.
This is one of the most important parts of the diagnostic process.
Celiac blood tests and biopsy findings are most reliable when a person is eating gluten regularly. NIDDK specifically notes that doctors do not recommend starting a gluten-free diet before diagnostic testing because it can affect results.
If you already stopped gluten, your doctor may discuss whether a gluten challenge is needed. This means reintroducing gluten for a period of time before testing, but it should be done under medical guidance.
Do not restart gluten on your own if symptoms are severe or if you have been advised against it.
Step 3: Celiac Disease Blood Tests
Blood testing is usually the first step.
The most common screening test is:
Tissue Transglutaminase IgA Antibody Test
This is often called the tTG-IgA test.
It looks for antibodies that are commonly elevated in people with celiac disease who are eating gluten. Mayo Clinic explains that serology testing looks for antibodies and that elevated levels of certain antibody proteins suggest an immune reaction to gluten.
The tTG-IgA test is widely used because it is accurate for many patients.
However, it is not perfect. That is why doctors often combine it with other information.
Step 4: Total IgA Level
A total IgA test is often ordered with tTG-IgA.
Why?
Some people have IgA deficiency. If a person has low IgA, the tTG-IgA test may be falsely negative.
NIDDK notes that IgA antibody tests are more sensitive for celiac disease, but IgG tests may be useful in people with IgA deficiency.
This is why a celiac panel may include more than one test.
Step 5: Additional Celiac Antibody Tests
Depending on the patient, doctors may order additional tests such as:
- Endomysial antibody test
- Deamidated gliadin peptide antibody test
- tTG-IgG test in selected cases
- DGP-IgG test in selected cases
These are not always needed for every patient.
The American College of Gastroenterology notes that older anti-gliadin or anti-gluten tests are no longer used for diagnosis and that saliva or stool antibody tests are not good substitutes for blood-based tests.
This matters because patients may find at-home or nonstandard “gluten tests” online that do not reliably diagnose celiac disease.
Step 6: Upper Endoscopy for Celiac Disease
If blood tests suggest celiac disease, an upper endoscopy may be recommended.
During an upper endoscopy, a gastroenterologist passes a thin flexible tube with a camera through the mouth to examine the upper digestive tract. The patient is usually sedated for comfort.
The doctor can look at the esophagus, stomach, and beginning of the small intestine.
For celiac disease, the most important part is the small-intestinal biopsy.
Step 7: Small-Intestinal Biopsy
A biopsy means taking tiny tissue samples.
In suspected celiac disease, samples are usually taken from the duodenum, which is the first part of the small intestine. A pathologist then examines the tissue under a microscope.
The biopsy may show:
- Villous atrophy
- Increased inflammatory cells
- Changes in the small-intestinal lining
- Damage consistent with celiac disease
Cleveland Clinic describes celiac testing as usually involving both blood testing for antibodies and biopsy to look for damage to the intestinal lining.
A biopsy can help confirm the diagnosis and rule out other causes of symptoms.
Why Biopsy Matters
Some patients ask, “If my blood test is positive, do I still need endoscopy?”
The answer depends on the patient, the test results, the doctor’s judgment, and clinical guidelines.
In many adults, biopsy confirmation is still commonly used because it provides direct evidence of intestinal damage. It may also help identify other problems if symptoms are not due only to celiac disease.
Endoscopy can be especially helpful when:
- Blood tests are positive
- Symptoms are severe
- There is weight loss
- There is anemia
- The diagnosis is uncertain
- Symptoms do not match blood test results
- Another upper GI condition is possible
Step 8: Genetic Testing
Genetic testing may be used in selected cases, but it is not usually the first test.
Most people with celiac disease have HLA-DQ2 or HLA-DQ8 genes. However, having these genes does not mean a person definitely has celiac disease.
Many people have these genes and never develop the condition.
The bigger value of genetic testing is that a negative result can make celiac disease much less likely.
Genetic testing may be considered when:
- A patient already stopped gluten before testing
- Blood and biopsy results are unclear
- Family risk needs clarification
- The diagnosis is uncertain
- A patient had conflicting test results
Mayo Clinic notes that genetic testing may be used to help rule out celiac disease.
Step 9: Skin Biopsy for Dermatitis Herpetiformis
Some people with celiac disease develop a specific skin condition called dermatitis herpetiformis.
This rash is often:
- Itchy
- Blistering
- Symmetrical
- Found on elbows, knees, buttocks, scalp, or back
- Linked to gluten sensitivity in celiac disease
If dermatitis herpetiformis is suspected, a dermatologist may perform a skin biopsy. NIDDK notes that doctors may order skin biopsies in some cases to help diagnose celiac disease.
A confirmed diagnosis of dermatitis herpetiformis is strongly associated with celiac disease.
What If Blood Tests Are Negative?
Negative blood tests make celiac disease less likely, but they do not always end the evaluation.
A doctor may look at:
- Whether the patient was eating gluten during testing
- Whether total IgA was low
- Whether symptoms strongly suggest malabsorption
- Whether there is iron deficiency anemia
- Whether there is weight loss
- Whether there is family history
- Whether another test is needed
- Whether another diagnosis is more likely
If symptoms are persistent, a GI specialist may still evaluate for other digestive conditions.
What If Blood Tests Are Positive?
Positive celiac blood tests do not mean patients should start a gluten-free diet without a plan.
The next step may include:
- Reviewing the strength of antibody results
- Confirming current gluten intake
- Considering endoscopy with biopsy
- Checking nutritional deficiencies
- Discussing family screening
- Planning long-term management
A confirmed diagnosis allows the patient to understand the seriousness of the condition and follow the right treatment plan.
What If You Already Went Gluten-Free?
This is common.
Many patients remove gluten before seeing a doctor because they feel bloated, tired, or uncomfortable after meals.
The problem is that testing may become harder.
If you are already gluten-free, your doctor may discuss:
- How long you have avoided gluten
- Whether symptoms improved
- Whether you can safely reintroduce gluten
- Whether genetic testing is useful
- Whether endoscopy is appropriate
- Whether another diagnosis is more likely
Do not assume that feeling better on a gluten-free diet proves celiac disease. Gluten sensitivity, IBS, wheat intolerance, lower FODMAP intake, or other diet changes may also explain improvement.
What Is a Gluten Challenge?
A gluten challenge means eating gluten again before testing.
It may be recommended when a person stopped gluten before celiac disease was confirmed.
The goal is to trigger the immune response enough for blood tests or biopsy to detect it.
The exact amount and length of gluten exposure should be guided by a healthcare professional. This is not something patients should self-direct, especially if symptoms are severe.
Tests That Do Not Diagnose Celiac Disease Reliably
Not all gluten-related tests are medically reliable.
Be cautious with:
- Saliva antibody tests
- Stool antibody tests
- Hair analysis
- Food sensitivity panels
- Nonstandard online gluten tests
- IgG food intolerance panels
The American College of Gastroenterology warns that saliva or stool antibody tests are not good substitutes for blood-based testing.
If you suspect celiac disease, use medically accepted testing through a qualified healthcare provider.
Celiac Disease vs Gluten Sensitivity Testing
Celiac disease has specific blood tests and biopsy findings.
Non-celiac gluten sensitivity does not have one definitive diagnostic test.
This means gluten sensitivity is usually considered after:
- Celiac disease is ruled out
- Wheat allergy is ruled out
- Other GI conditions are considered
- Symptoms improve when gluten is removed
- Symptoms return when gluten is reintroduced
This is why celiac testing should happen first.
Celiac Disease vs Wheat Allergy Testing
Celiac disease is not the same as wheat allergy.
A wheat allergy involves an allergic immune reaction to wheat proteins. It may cause symptoms such as hives, swelling, breathing problems, vomiting, or even anaphylaxis in severe cases.
Celiac disease is autoimmune and primarily affects the small intestine.
Testing is different. Allergy testing does not diagnose celiac disease, and celiac antibody tests do not diagnose wheat allergy.
Who Should Consider Celiac Disease Testing?
Testing may be appropriate for people with:
- Chronic diarrhea
- Persistent bloating
- Abdominal pain
- Unexplained weight loss
- Iron deficiency anemia
- Low ferritin
- Chronic fatigue
- Greasy or foul-smelling stools
- Unexplained vitamin deficiencies
- Bone thinning or osteoporosis
- Mouth ulcers
- Dermatitis herpetiformis
- Family history of celiac disease
- Type 1 diabetes
- Autoimmune thyroid disease
- Elevated liver enzymes without a clear cause
The American Academy of Family Physicians’ summary of the ACG guideline states that symptomatic patients eating a gluten-containing diet should have serologic testing that includes tissue transglutaminase IgA and total IgA.
What Happens After Diagnosis?
If celiac disease is confirmed, treatment usually includes a strict gluten-free diet.
This means avoiding:
- Wheat
- Barley
- Rye
- Regular bread
- Regular pasta
- Many baked goods
- Some cereals
- Beer
- Some sauces and processed foods
Follow-up may include:
- Nutrient testing
- Iron studies
- Vitamin D levels
- B12 or folate testing
- Bone health evaluation in selected patients
- Dietitian support
- Repeat antibody testing
- Monitoring symptom improvement
NIDDK states that people with celiac disease need to follow a gluten-free diet for life.
Why Follow-Up Matters
A diagnosis is not the end of care.
Follow-up helps confirm that:
- Symptoms are improving
- Antibody levels are decreasing
- Nutrient deficiencies are corrected
- The patient understands hidden gluten sources
- Accidental gluten exposure is minimized
- The small intestine is healing
Some patients continue to have symptoms even after going gluten-free. In those cases, doctors may look for hidden gluten exposure, IBS, lactose intolerance, SIBO, microscopic colitis, inflammatory bowel disease, or another condition.

When to See a Gastroenterologist
You should see a gastroenterologist if you have symptoms that suggest celiac disease or if your blood work shows unexplained nutrient problems.
Important reasons to seek GI evaluation include:
- Chronic bloating
- Long-term diarrhea
- Recurrent constipation with abdominal pain
- Unexplained anemia
- Low ferritin
- Unexplained weight loss
- Persistent nausea
- Fatigue with nutrient deficiencies
- Family history of celiac disease
- Symptoms after eating gluten
- Symptoms that continue despite diet changes
For patients in Houston, Cypress, Katy, or Jersey Village, GastroDoxs can evaluate persistent digestive symptoms, order appropriate testing, and determine whether endoscopy or biopsy is needed.
Final Answer: How Is Celiac Disease Diagnosed?
Celiac disease is diagnosed through a combination of symptom review, blood tests, and sometimes upper endoscopy with small-intestinal biopsy.
The most common first tests include tTG-IgA and total IgA. If results suggest celiac disease, a gastroenterologist may recommend an upper endoscopy with biopsy to confirm small-intestinal damage.
Testing should be done while the patient is still eating gluten. Starting a gluten-free diet before testing can make celiac disease harder to diagnose.


