








Hemorrhoids are one of the most common reasons people search for answers about rectal bleeding, anal pain, itching, swelling, and painful bowel movements. They are also one of the most misunderstood digestive problems online. Many people assume every episode of bright red blood is a hemorrhoid. Others believe hemorrhoids are always painful, always external, or always caused by poor hygiene. None of those assumptions is fully accurate.
A better starting point is this: hemorrhoids are swollen and inflamed veins in the lower rectum or around the anus. They can be internal or external. Some bleed without causing pain. Others cause itching, tenderness, lump-like swelling, or sharp discomfort when sitting or wiping. Some improve with fiber, hydration, and time. Others need office treatment or surgery. And sometimes the symptom that a person calls “hemorrhoids” turns out to be something else entirely.
That is why hemorrhoids deserve a serious, well-structured explanation. This guide covers what hemorrhoids are, the difference between internal and external hemorrhoids, what bleeding usually means, common causes, best at-home treatments, when a doctor should evaluate symptoms, and when rectal bleeding should not be dismissed.
Hemorrhoids are enlarged, swollen veins in and around the anus and lower rectum. Internal hemorrhoids form inside the rectum and often cause painless bright red bleeding. External hemorrhoids form under the skin around the anus and are more likely to cause itching, pain, swelling, or a tender lump. Some hemorrhoids improve with home care such as more fiber, fluids, warm baths, and short-term over-the-counter treatment. More severe or persistent cases may need office procedures such as rubber band ligation or, less commonly, surgery.
Hemorrhoids sit in a body area where several conditions can create overlapping symptoms. Bright red blood may come from internal hemorrhoids, but it can also come from anal fissures, proctitis, colorectal polyps, rectal cancer, inflammatory bowel disease, or other sources. Pain with bowel movements may point to external hemorrhoids, but severe pain can also occur with a thrombosed hemorrhoid or an anal fissure. Itching can happen with hemorrhoids, but also with dermatitis, moisture irritation, infections, or chronic diarrhea.
That overlap is why symptom clusters matter more than labels. A person may say, “I know it is just hemorrhoids,” but the real question is whether the overall pattern fits hemorrhoids well enough to avoid missing another diagnosis..
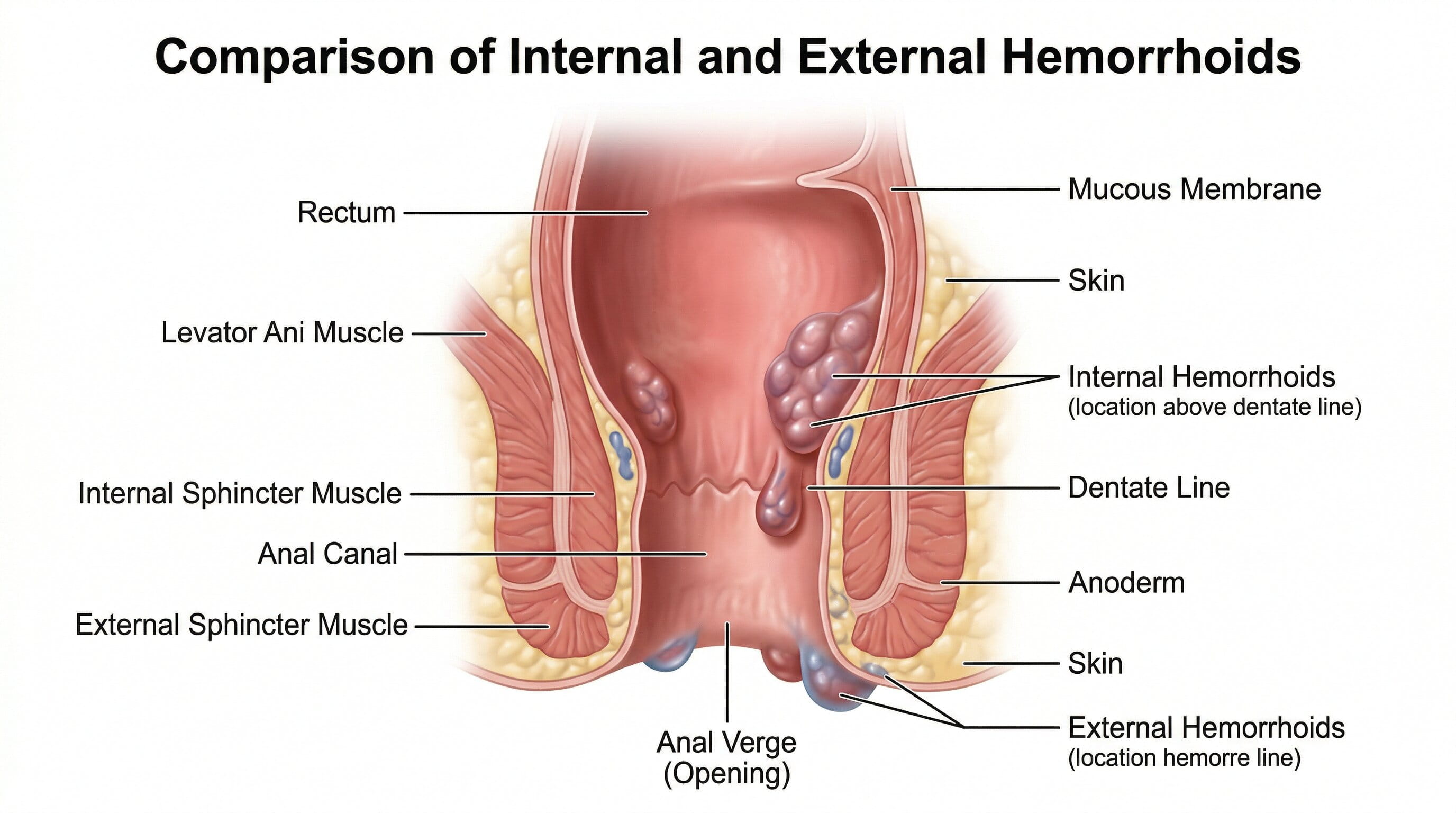
Understanding the difference between internal and external hemorrhoids is essential because the symptoms, treatment choices, and pain patterns are not the same.
Internal hemorrhoids form in the lining of the anus and lower rectum. They are usually not painful because they occur in an area with fewer pain-sensitive nerves. The most common symptom is bright red bleeding during or after a bowel movement. Some people also notice tissue bulging or protruding outside the anus during a bowel movement. This is called prolapse.
Internal hemorrhoids can be described by grade:
Grading matters because lower-grade internal hemorrhoids often respond well to fiber and office treatment, while more advanced prolapse may require procedural care.
External hemorrhoids form under the skin around the anus. Because this area has more pain-sensitive nerves, external hemorrhoids are more likely to cause discomfort. Symptoms may include:
If a clot forms inside an external hemorrhoid, it becomes a thrombosed hemorrhoid. That can cause sudden, significant pain and a firm bluish or purple lump.
One of the highest-volume hemorrhoid questions in search is some version of: “What kind of bleeding do hemorrhoids cause?”
Typical hemorrhoid bleeding is usually:
That said, bleeding alone does not prove hemorrhoids. Even when hemorrhoids are present, bleeding may still need evaluation if it is persistent, heavy, recurrent, associated with abdominal pain, accompanied by changes in bowel habits, or happening in someone who is due for colorectal cancer screening.
Usually no. Black, tar-like stools more often suggest bleeding from higher up in the gastrointestinal tract and need medical attention. Darker blood can also have other causes. Hemorrhoid bleeding is more typically bright red.
Hemorrhoid symptoms vary by type and severity. Common symptoms include:
One important clinical clue is that internal hemorrhoids often bleed but do not hurt much, while external hemorrhoids are more likely to hurt or itch.
Hemorrhoids are linked to increased pressure and straining in the anorectal area. Several common factors can contribute.
This is one of the most common triggers. Repeated straining and passing hard stool can irritate the anal canal and worsen hemorrhoidal swelling.
Spending too much time on the toilet can increase pressure in the hemorrhoidal veins. This is one reason clinicians often advise shorter, more efficient bathroom habits.
A low-fiber diet contributes to harder stools, irregular bowel movements, and more straining.
Pregnancy can increase pressure in the pelvic and rectal veins, and constipation is also common during pregnancy. As a result, hemorrhoids are very common in pregnancy and after delivery.
Not all hemorrhoids are tied to constipation. Frequent loose stools, repeated wiping, and irritation can also worsen hemorrhoid symptoms.
Supporting tissues in the anal canal can weaken over time, which may contribute to hemorrhoid symptoms in older adults.
Anything that repeatedly increases abdominal and pelvic pressure may aggravate hemorrhoids.
Pregnancy-related hemorrhoid queries are common because symptoms often appear suddenly in the second or third trimester or after labor. Several factors come together at once:
Most pregnancy-related hemorrhoids improve with conservative care, but persistent bleeding or severe pain should still be evaluated.
Yes, especially external hemorrhoids or thrombosed external hemorrhoids. However, severe sharp pain during bowel movements can also point to an anal fissure. That distinction matters.
A fissure is a small tear in the lining of the anus. It often causes intense cutting or tearing pain during and after bowel movements, sometimes with bright red blood. Patients often call this “hemorrhoids,” but the treatment approach can differ.
A thrombosed hemorrhoid is an external hemorrhoid that develops a blood clot. It often causes:
This is one of the more urgent hemorrhoid-related scenarios because timely medical evaluation may provide more rapid relief in selected cases.
A hemorrhoid diagnosis usually starts with a medical history and physical exam. For external hemorrhoids, the diagnosis may be visible on exam. For internal hemorrhoids, the evaluation may include a digital rectal exam and a look inside the anal canal and lower rectum.
Depending on age, symptoms, risk factors, or bleeding pattern, further evaluation may be recommended. This does not always mean something dangerous is present. It means rectal bleeding deserves the right level of caution.
More evaluation may be appropriate when:
The point is not to alarm patients. The point is to avoid assuming every bleeding episode is automatically benign.
Patients frequently confuse these two conditions.
This distinction matters because severe pain is often more suggestive of fissure or thrombosis than simple internal hemorrhoids.
Another major search theme is whether hemorrhoids can turn into cancer. The answer is no. Hemorrhoids do not cause colorectal cancer and do not increase the risk of colorectal cancer. But the symptoms can overlap enough that evaluation is sometimes needed to rule out something more serious.
Symptoms that should not be casually blamed on hemorrhoids include:
A good rule is this: hemorrhoids are common, but “common” should never become a reason to ignore persistent bleeding.
Mild hemorrhoids often improve with conservative care. The most effective home-based plan is usually centered on making bowel movements easier and less traumatic.
Fiber helps soften stool and reduce straining. This can improve both symptoms and prevention. Food sources include fruits, vegetables, beans, lentils, oats, bran, and whole grains. Some patients also benefit from fiber supplements.
Fluids help fiber work better. Hydration supports softer stools and more comfortable bowel movements.
Straining worsens pressure in the hemorrhoidal veins. Do not force a bowel movement and do not sit waiting on the toilet for long periods.
Bathroom habits matter. Sitting on the toilet too long, especially while scrolling on a phone, can worsen symptoms.
Warm water baths for the anal area can help soothe irritation and reduce discomfort.
Over-the-counter creams, ointments, pads, or suppositories may reduce mild pain, swelling, or itching for a short period. These products are generally meant for short-term symptom relief rather than indefinite use.
Over-wiping and aggressive cleaning can make symptoms worse. Gentle cleansing and avoiding excessive rubbing can help reduce irritation.
The best hemorrhoid diet is usually one that makes stools soft, regular, and easier to pass. Helpful foods often include:
The goal is not a trendy “hemorrhoid detox.” The goal is consistent bowel regularity.
There is no universal hemorrhoid food blacklist, but symptoms may worsen when bowel habits become irregular. Common problems include:
Some people also notice temporary worsening with spicy foods, but this is variable and not the main driver for most patients.
Home treatment is reasonable for mild symptoms, but medical care is a good idea when:
When symptoms persist, several office procedures may be considered for internal hemorrhoids.
A small band is placed around the base of the internal hemorrhoid to cut off blood supply so the tissue shrinks and falls away. This is one of the most commonly used office treatments.
Heat-based treatment can help shrink smaller internal hemorrhoids.
A solution is injected into the hemorrhoid to shrink it.
These options are generally for internal hemorrhoids, not external hemorrhoids.
Surgery is usually reserved for more severe cases, such as large symptomatic hemorrhoids, recurrent bleeding, significant prolapse, mixed internal and external disease, or cases that do not respond to less invasive measures.
Surgical options may include hemorrhoidectomy or other procedure-based approaches depending on anatomy and severity.
Mild hemorrhoid flares may improve within days to a couple of weeks, especially when constipation and straining are corrected. But that timeline varies widely. Hemorrhoids tend to recur when the underlying bowel pattern does not change.
This is why short-term symptom relief is not enough. Long-term control usually comes from preventing repeat straining, reducing constipation, and treating persistent internal hemorrhoids when needed.
Recurrent hemorrhoids are common because the underlying triggers often remain in place. A person may use a cream, feel better for a week, and then return to the same pattern of low fiber, constipation, long toilet sitting, frequent straining, or repeated irritation.
The real prevention plan is behavioral as much as it is medical.
To prevent hemorrhoids from recurring, consider these habits:
These changes are not glamorous, but they are often the most effective long-term strategy.
Seek urgent medical care if bleeding is heavy, persistent, associated with dizziness, faintness, severe abdominal pain, fever, or significant weakness. Black stools or maroon stool should not be assumed to be hemorrhoids. Severe anal pain with bleeding also deserves prompt evaluation.

A gastroenterologist or colorectal specialist may be involved when bleeding is recurrent, symptoms are severe, the diagnosis is not clear, or endoscopic evaluation is needed. Patients who are age 45 or older, or who have other colorectal cancer risk factors, may also need screening based on current preventive care guidance.
For patients with rectal bleeding, painful bowel movements, or ongoing anorectal symptoms, GastroDoxs can help evaluate whether the problem fits hemorrhoids, fissure, or another GI condition and guide next-step care.
False. Internal hemorrhoids often bleed without much pain.
False. Bright red blood can have multiple causes.
False. Hemorrhoids do not cause colorectal cancer.
Not usually. Creams may relieve symptoms, but prevention usually depends on stool consistency and bowel habits.
Also false. Intermittent symptoms can still deserve evaluation, especially if bleeding keeps returning.
Hemorrhoids are common, but they should not be oversimplified. Internal hemorrhoids often cause painless bright red bleeding. External hemorrhoids are more likely to cause pain, itching, swelling, or a tender lump. Thrombosed hemorrhoids can be intensely painful. Many mild cases improve with fiber, fluids, warm baths, and better toilet habits. Persistent bleeding, significant pain, prolapse, or symptoms that do not fit a straightforward hemorrhoid pattern should be evaluated.
The most important takeaway is this: rectal bleeding should not be ignored just because hemorrhoids are common. The right diagnosis matters, and early evaluation helps patients get the right treatment sooner.
Dr. Bharat Pothuri is a Board-Certified Gastroenterologist and Hepatologist. With extensive experience in digestive health, he specializes in advanced endoscopic procedures, chronic GI disorder management, and preventive care. Dr. Pothuri is dedicated to providing expert, patient-focused insights to help improve gut health and overall well-being.
External hemorrhoids may appear as swollen or tender lumps around the anus. Internal hemorrhoids usually are not visible unless they prolapse.
No. Some hemorrhoids itch, swell, or hurt without obvious bleeding.
Internal hemorrhoids are often painless. External hemorrhoids and thrombosed hemorrhoids can be painful.
Persistent bleeding, changes in bowel habits, weight loss, anemia, abdominal pain, or symptoms that do not improve need medical evaluation.
A combination of softer stools, more fiber, hydration, warm baths, avoiding straining, and short-term over-the-counter symptom relief is often the quickest conservative approach.
Mild hemorrhoids often improve, especially when constipation and straining are corrected. Recurrent cases may need formal treatment.
If bleeding lasts more than a day or two, symptoms persist after about a week of home care, or pain is severe, it is a good idea to get evaluated.


