Colitis means inflammation in the colon. Crohn’s disease is a chronic inflammatory bowel disease that can affect any part of the digestive tract, from the mouth to the anus. Crohn’s can involve the colon, but it can also affect the small intestine and deeper layers of the bowel wall. That is the central difference.
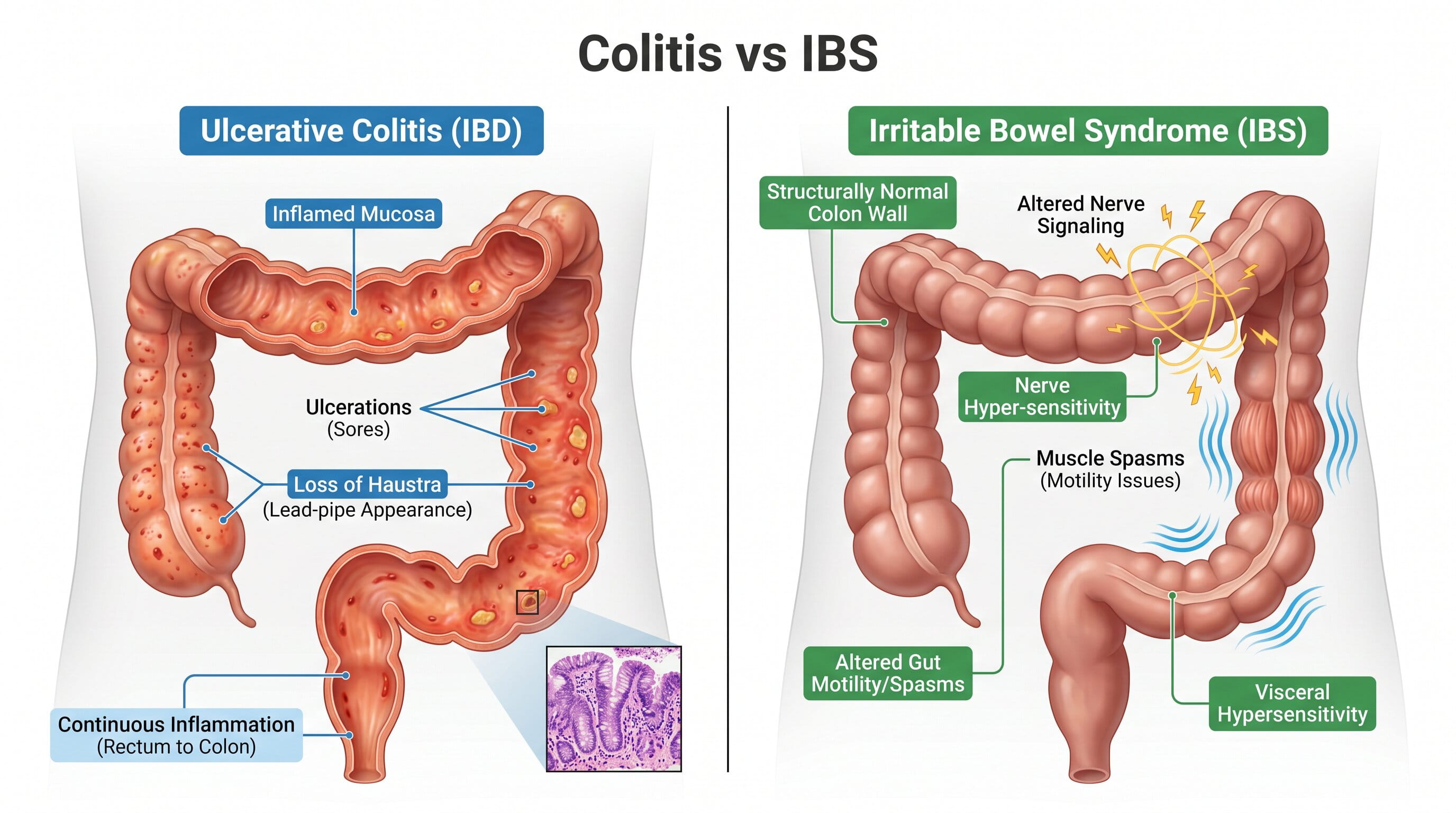
Ulcerative colitis, one major form of colitis, affects the colon and rectum. It usually begins in the rectum and can extend continuously through the colon. Crohn’s disease often appears in patches and may spare areas between inflamed segments. Because symptoms overlap, a gastroenterologist often uses colonoscopy, biopsies, stool tests, blood work, and imaging to tell them apart.
This patient-facing article is written for people who want a clear answer before they schedule care. It does not replace a diagnosis. Symptoms such as rectal bleeding, severe pain, dehydration, fever, or ongoing diarrhea should be discussed with a qualified clinician. GastroDoxs can help patients with persistent bowel changes understand whether symptoms may be related to colon inflammation, infection, inflammatory bowel disease, hemorrhoids, medication effects, or another digestive condition.
Why Patients Confuse Colitis and Crohn’s Disease
The confusion is understandable. Both conditions can cause diarrhea, abdominal pain, rectal bleeding, fatigue, urgency, weight loss, and flare-ups. Both are discussed under the larger inflammatory bowel disease category when the colitis is ulcerative colitis. Both can also affect a patient’s work, travel, eating habits, sleep, and emotional health.
The words add to the confusion. “Colitis” sounds like a disease name, but it is also a descriptive term. It simply means colon inflammation. Crohn’s disease is a specific chronic inflammatory condition. A person can have Crohn’s disease involving the colon, sometimes called Crohn’s colitis. A person can also have ulcerative colitis, infectious colitis, ischemic colitis, microscopic colitis, or another form.
This is why search intent matters. When patients ask “colitis vs Crohn’s disease,” they are usually asking whether their symptoms sound temporary, chronic, autoimmune, infectious, or serious. The answer depends on pattern, location, test results, and severity.
What Colitis Means
Colitis means the colon lining is inflamed. The colon is responsible for absorbing water, moving stool, and storing waste before a bowel movement. Inflammation can make the colon more sensitive and less effective at absorbing water. This can lead to loose stool, urgency, mucus, pain, and bleeding.
Different causes can inflame the colon. Infection may inflame the colon for days or weeks. Ulcerative colitis can cause chronic inflammation with flare-ups and remission. Microscopic colitis can cause chronic watery diarrhea that may only be diagnosed after biopsies. Ischemic colitis happens when blood flow to the colon is reduced.
The word “colitis” should lead to the next question: what type? The type determines treatment, monitoring, and long-term risk.
What Crohn’s Disease Means
Crohn’s disease is a chronic inflammatory bowel disease. It can affect the digestive tract in different locations. The end of the small intestine and the beginning of the colon are common areas, but Crohn’s can occur elsewhere. Inflammation can extend deeper into the bowel wall, which is one reason Crohn’s can lead to complications such as narrowing, fistulas, abscesses, or malnutrition.
Crohn’s symptoms vary based on location. Small bowel Crohn’s may cause pain, diarrhea, weight loss, fatigue, nutrient problems, or obstruction-like symptoms. Crohn’s involving the colon may cause diarrhea, urgency, bleeding, and cramps that look similar to colitis.
Because Crohn’s may affect areas beyond the reach of a standard colonoscopy, imaging or capsule-type evaluation may be considered in selected patients.
Location of Inflammation
Location is one of the most useful differences. Ulcerative colitis affects the colon and rectum. It does not involve the small intestine except for limited backwash inflammation in some cases. Crohn’s disease can affect the small intestine, colon, rectum, anus, stomach, or other parts of the digestive tract.
This matters because symptoms may point to location. Rectal inflammation may cause urgency, bleeding, and tenesmus. Small intestine inflammation may cause weight loss, malnutrition, cramping, or anemia. Perianal Crohn’s disease may cause fissures, fistulas, drainage, or abscesses.
- Ulcerative colitis: colon and rectum.
- Crohn’s disease: any part of the digestive tract.
- Crohn’s colitis: Crohn’s disease affecting the colon.
- Microscopic colitis: colon inflammation seen on biopsy.
- Infectious colitis: colon inflammation from infection.
Pattern of Inflammation
Ulcerative colitis often has a continuous pattern. It usually starts in the rectum and extends upward through the colon without normal areas in between. This continuous pattern helps doctors distinguish it from Crohn’s disease.
Crohn’s disease often has skip areas, meaning inflamed segments may be separated by normal tissue. Crohn’s may also involve deeper layers of the bowel wall, while ulcerative colitis is typically limited to the inner lining of the colon.
No single symptom confirms this pattern. Colonoscopy and biopsies are important because the pattern can be seen and sampled.
Symptom Comparison
Both conditions may cause diarrhea and abdominal pain. Ulcerative colitis often produces bloody diarrhea, urgency, mucus, rectal pressure, and frequent bowel movements. Crohn’s disease may cause diarrhea, cramping, fatigue, weight loss, and malnutrition. Bleeding can happen in Crohn’s disease, especially when the colon is involved, but the pattern may vary.
Crohn’s disease may also cause symptoms related to narrowing or deeper inflammation, such as cramping after meals, nausea, vomiting, or obstruction-like episodes. Perianal symptoms such as fistulas or abscesses can suggest Crohn’s disease.
Because symptoms overlap, patients should avoid self-diagnosing based on one feature. Blood in stool, diarrhea, and abdominal pain need context.
How Diagnosis Is Made
Diagnosis begins with careful history. A gastroenterologist asks about stool frequency, blood, mucus, pain location, nighttime symptoms, weight loss, fever, family history, medications, travel, antibiotics, and prior testing.
Blood work may check for anemia, inflammation, nutritional issues, and general health. Stool tests may check infection, inflammation, or hidden blood. Colonoscopy helps evaluate the colon lining and terminal ileum when possible. Biopsies can identify chronic inflammation and microscopic patterns.
If Crohn’s disease is suspected beyond the colon, additional imaging may be needed. This may help evaluate the small intestine, strictures, fistulas, or complications that colonoscopy alone may not fully assess.
Complications to Understand
Uncontrolled colon inflammation can lead to bleeding, anemia, dehydration, severe flare-ups, and increased colon cancer risk over time in some chronic inflammatory bowel disease patients. Crohn’s disease can additionally cause strictures, fistulas, abscesses, and nutrient deficiencies depending on location and severity.
Complications are not meant to frighten patients. They are the reason early evaluation and treatment matter. The goal is to control inflammation before it causes damage, hospital visits, or quality-of-life decline.
Patients should seek urgent care for heavy bleeding, severe pain, high fever, dehydration, vomiting with inability to keep fluids down, fainting, or a rigid swollen abdomen.

Treatment Approach
Treatment depends on the exact diagnosis. Ulcerative colitis and Crohn’s disease both may involve medications that reduce inflammation and maintain remission. Options vary from topical therapy to oral medications, immune-modifying drugs, biologic therapy, targeted small molecules, nutrition support, and sometimes surgery.
Not every colitis case needs IBD medication. Infectious colitis may require different care. Microscopic colitis has its own treatment pathway. Ischemic colitis requires cause-based assessment. This is why a label such as “colitis” should be followed by a clear explanation of type, location, severity, and next steps.
At GastroDoxs, patients with persistent diarrhea, rectal bleeding, urgency, and abdominal pain can be evaluated for the cause of inflammation instead of guessing based on symptoms alone.
Patient Takeaway
Colitis describes colon inflammation. Crohn’s disease is a chronic inflammatory bowel disease that can involve more than the colon and may affect deeper bowel layers. The two can look similar when Crohn’s affects the colon, but they are not identical.
The safest next step is evaluation when symptoms include bleeding, persistent diarrhea, weight loss, fever, nighttime diarrhea, anemia, or recurring flare-ups. Diagnosis is not only about naming the condition. It is about choosing the right treatment and protecting long-term digestive health.
Additional Patient Guidance for Better Decision-Making
A helpful way to prepare for a gastroenterology visit is to write down your normal bowel pattern and then compare it with what is happening now. Include the number of bowel movements per day, stool appearance, bleeding, urgency, nighttime symptoms, fever, pain level, weight changes, recent travel, recent antibiotics, and any medication or supplement changes. This information helps separate short-term irritation from a pattern that may suggest inflammation or infection.
Patients often focus on one symptom, but clinicians look for combinations. Diarrhea alone has many causes. Diarrhea plus blood, fever, nighttime symptoms, or weight loss is more concerning. Abdominal pain alone may be common, but pain plus severe tenderness, vomiting, dehydration, or a rigid abdomen can change the level of urgency. The full pattern matters more than one isolated symptom.
Do not rely only on diet changes when warning signs are present. Food can influence symptoms, but food is not the only explanation for colon inflammation. Infection, inflammatory bowel disease, medication effects, ischemia, microscopic inflammation, hemorrhoids, fissures, polyps, and other conditions may require different care. A correct diagnosis helps prevent both overtreatment and undertreatment.
At GastroDoxs, the patient goal is clarity. The right evaluation can explain whether symptoms are likely functional, inflammatory, infectious, medication-related, vascular, or structural. Once the cause is clearer, care can be built around symptom relief, inflammation control, prevention of complications, and a practical plan for what to do if symptoms return.
Another practical step is to avoid self-labeling the condition before testing. Many colon problems share the same surface symptoms. A patient may say “colitis,” “IBS,” “flare,” or “food poisoning,” but the treatment path changes when stool tests, blood work, colonoscopy findings, biopsies, medication history, or imaging reveal the real cause. Accurate naming is part of safe care.
Patients should also think about duration. A one-day bowel change after a rich meal is different from two weeks of diarrhea. One small spot of blood after straining is different from repeated blood mixed with stool. A symptom that disappears quickly may still be worth mentioning, but a symptom that repeats or escalates should move higher on the priority list.
If bowel symptoms are changing your routine, limiting travel, causing embarrassment, or making you check for the nearest restroom before leaving home, that is enough reason to seek guidance. Early evaluation often gives patients more options and less uncertainty.