Adenomas are usually not cancer, but many are considered precancerous. This means the cells have abnormal growth patterns that could progress toward cancer over time. Risk is higher when an adenoma is large, multiple, villous, high-grade dysplastic, or incompletely removed.
Precancerous Does Not Mean Cancer
The word precancerous can frighten patients. It should be understood as a risk category, not a cancer diagnosis. A precancerous adenoma has abnormal cells that may develop further changes over time. Removing the adenoma helps stop that process. This is why colonoscopy is preventive rather than only diagnostic.
How Adenomas Can Progress
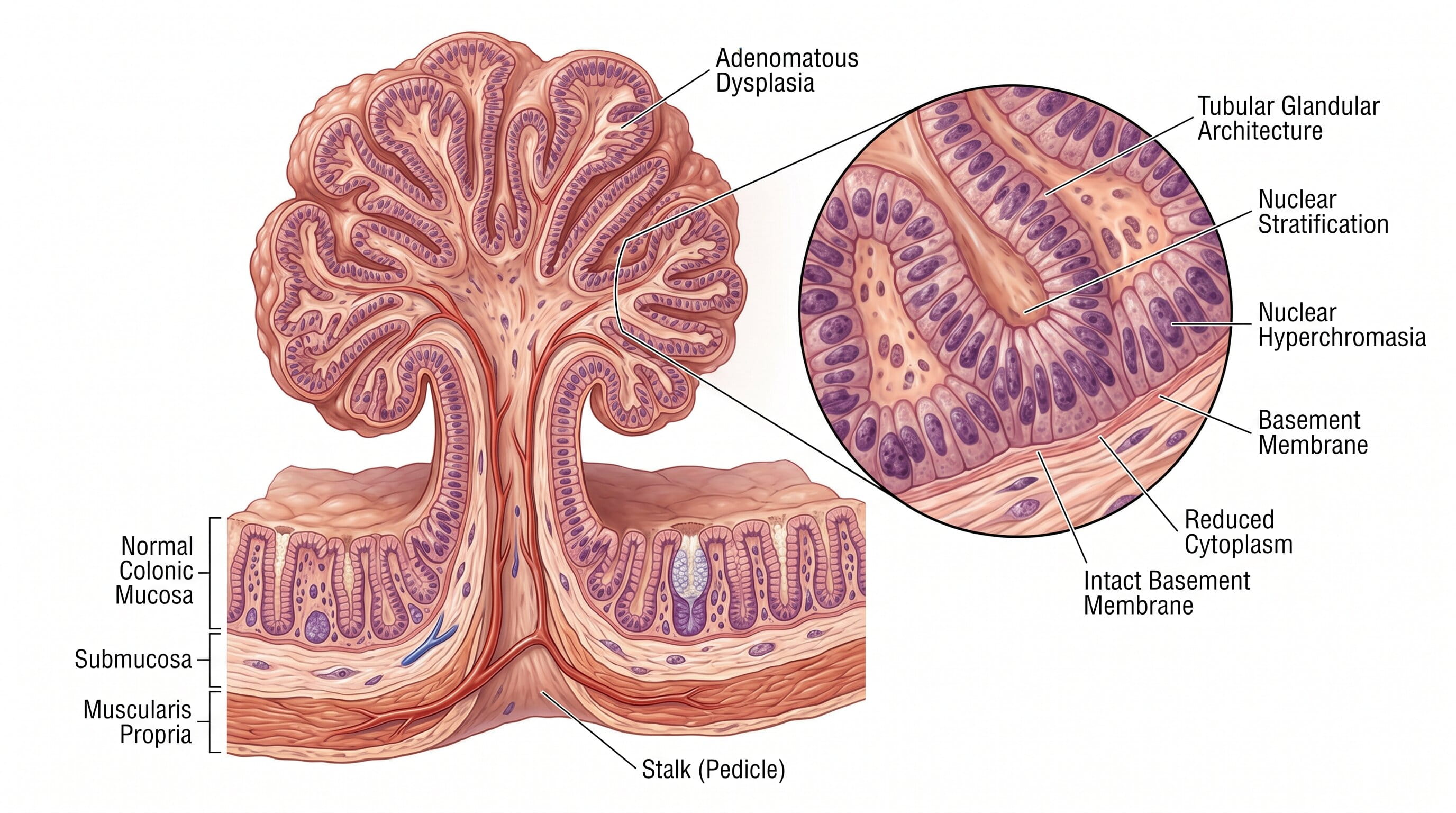
Some colorectal cancers develop through a gradual sequence from normal lining to adenoma to advanced adenoma to cancer. This pathway often takes years, which creates a window for screening and removal. Not every adenoma will become cancer. Many never progress. The challenge is that doctors cannot safely predict which individual adenoma would become cancer if left in place, so removal is the standard preventive approach.
Features That Raise Concern
Cancer risk rises with larger size, higher number of adenomas, villous or tubulovillous architecture, high-grade dysplasia, and suspicious endoscopic features. An adenoma 10 mm or larger is more concerning than a tiny lesion. Multiple adenomas suggest a stronger tendency for polyp formation. High-grade dysplasia means cells are more abnormal, though it still does not automatically mean invasive cancer.
Low-Grade vs High-Grade Dysplasia
Low-grade dysplasia is common in adenomas and reflects early abnormal cell changes. High-grade dysplasia is more advanced and usually leads to closer follow-up. The distinction is made by pathology. Patients should not interpret the phrase dysplasia without discussing the full report, because dysplasia grade, size, and removal completeness all matter.
What Happens If Cancer Is Found
If pathology shows invasive cancer, the plan changes. The gastroenterologist may refer the patient for staging, imaging, surgery consultation, oncology input, or advanced endoscopic assessment depending on depth and margins. This is different from routine adenoma care. Most adenomas removed during screening are not invasive cancer, but pathology is essential to confirm.
Why Complete Removal Matters
Complete removal is central to risk reduction. Incomplete resection can leave tissue behind. Large, flat, or piecemeal lesions may need earlier follow-up to confirm the site is clear. Patients should ask whether the adenoma was completely removed and whether any special surveillance is needed.
Screening Age and Risk
Average-risk colorectal cancer screening commonly starts at age 45, but earlier evaluation may be needed for family history, prior advanced adenomas, hereditary syndromes, inflammatory bowel disease, or symptoms. Screening finds adenomas before they become cancer, which is the core benefit

When to See a Gastroenterologist
See a gastroenterologist if your report says advanced adenoma, high-grade dysplasia, villous features, large adenoma, multiple adenomas, or incomplete removal. At GastroDoxs, patients in Cypress, Katy, Jersey Village, and Greater Houston can receive colonoscopy-based evaluation, polyp removal, and follow-up planning from a digestive health team led by Dr. Bharat Pothuri.
How to Read the Colonoscopy and Pathology Reports
For are adenomas cancerous? understanding precancerous risk, the colonoscopy report and pathology report should be read together. The colonoscopy report usually documents location, size, shape, removal method, bowel preparation quality, and whether the exam reached the intended portion of the colon. The pathology report confirms tissue type and dysplasia. Patients should not rely on memory alone because small details can change follow-up timing. A report that says one small tubular adenoma is different from a report that lists a large adenoma, multiple adenomas, villous features, high-grade dysplasia, or piecemeal resection. Keeping these reports helps future doctors avoid repeating tests too early or waiting too long.
Patient Questions That Improve Follow-Up
The best visit after an adenoma finding should end with clear answers. Patients can ask: What type of adenoma or serrated lesion was found? How many were removed? What was the largest size? Was removal complete? Did the pathology show dysplasia? Was the bowel prep good enough? When should the next colonoscopy happen? Does my family history change the plan? These questions make the visit more useful and support safer long-term prevention. They also reduce anxiety because the patient understands why the follow-up interval was chosen.
Lifestyle and Risk Reduction After an Adenoma
Lifestyle changes cannot remove an adenoma that already exists, but they can support future risk reduction. Practical steps include staying current with colonoscopy surveillance, avoiding tobacco, limiting alcohol, maintaining a healthy weight, increasing physical activity, and choosing a diet pattern that includes fiber-rich foods, fruits, vegetables, and fewer processed meats. Patients should also manage diabetes, inflammatory bowel disease, and other medical conditions with their clinicians. The goal is not perfection. The goal is to combine medical prevention with realistic habits that support colon health over time.
Warning Signs That Need Prompt Medical Attention
Contact a healthcare professional promptly if you have any of the following:
- Rectal bleeding or black stools
- New or unexplained iron deficiency anemia
- Unintentional weight loss
- Persistent change in bowel habits
- Family history of colorectal cancer or advanced polyps
- A positive stool-based screening test
- Abdominal pain with vomiting, fever, or worsening weakness
GastroDoxs Care Note
At GastroDoxs, patients in Cypress, Katy, Jersey Village, and Greater Houston can receive colonoscopy-based evaluation, polyp removal, and follow-up planning from a digestive health team led by Dr. Bharat Pothuri.
Key Takeaways
Adenoma is not the same as cancer, but it should not be ignored. It is a marker of future risk and a chance to prevent colorectal cancer. The safest plan is removal, pathology review, risk-based surveillance, and prompt evaluation of any new warning symptoms.